Abstract
OBJECTIVE: The goal of this study was to determine the epidemiology of injuries associated with nursery products among young children treated in US emergency departments.
METHODS: Data from the National Electronic Injury Surveillance System were retrospectively analyzed for patients aged <3 years who sustained an injury associated with a nursery product from 1991 through 2011.
RESULTS: An estimated 1 391 844 (95% confidence interval, 1 169 489–1 614 199) nursery product–related injuries among children aged <3 years were treated in US emergency departments during the 21-year study period, averaging 56.29 injuries per 10 000 children. The annual injury rate decreased significantly by 33.9% from 1991 to 2003, followed by a significant increase of 23.7% from 2003 to 2011. The decrease was driven by a significant decline in baby walker/jumper/exerciser-related injuries; the increase was driven by a significant increase in concussions and closed head injuries. Nursery product–related injuries were most commonly associated with baby carriers (19.5%), cribs/mattresses (18.6%), strollers/carriages (16.5%), or baby walkers/jumpers/exercisers (16.2%). The most common mechanism of injury was a self-precipitated fall (80.0%), and the most frequently injured body region was the head or neck (47.1%).
CONCLUSIONS: Although successful injury prevention efforts with baby walkers led to a decline in nursery product–related injuries from 1991 to 2003, the number and rate of these injuries have been increasing since 2003. Greater efforts are warranted to prevent injuries associated with other nursery products, especially baby carriers, cribs, and strollers. Prevention of falls and concussions/closed head injuries associated with nursery products also deserves special attention.
- CHI —
- closed head injury
- CI —
- confidence interval
- CPSC —
- United States Consumer Product Safety Commission
- ED —
- emergency department
- NEISS —
- National Electronic Injury Surveillance System
- RR —
- relative risk
What’s Known on This Subject:
Previous studies have described the epidemiology of injuries associated with specific nursery products, such as cribs and baby walkers. No study has attempted to examine and compare classes of nursery products by using a nationally representative sample.
What This Study Adds:
This study is the first to use nationally representative data to investigate the epidemiology of injuries associated with a broad range of nursery products among young children. The rise in these injuries since 2003 warrants increased injury prevention efforts.
Nearly every household in the United States with a newborn or young child uses nursery products, which include infant furniture, barriers, walkers, devices, and equipment used for transporting, bathing, or caring for a child. These products are intended to help parents raise their children. However, nursery products can pose a threat to the well-being of young children, especially if the products do not meet current safety standards. From 2009 to 2012, nursery products were the leading category of children’s products recalled in the United State,1–4 and they account for millions of dangerous products found in US households.5,6 Nursery products are known to be a source of child injuries7 and deaths.8,9 In 2014, there were 69 300 emergency department (ED) visits by children <5 years old attributable to nursery products.10
Few studies have evaluated injuries associated with multiple classes of nursery products among infants and children, including 1 small study in a non-US population.11 Most previous epidemiologic studies focus on injuries associated with 1 or several products in a single product class, such as strollers,12–14 cribs,15 baby walkers,16–20 and baby bottles,21 using both regional and national data.
Nursery product safety is a critical yet challenging issue in injury prevention, complicated by the rapid anatomic, motor, and cognitive development of young children as well as injury profiles unique to specific products based on their design and use.15,22 Identification of injury characteristics and patterns associated with nursery products is therefore essential in pinpointing areas of greatest concern for caregivers, health care providers, manufacturers, and policy makers. The objective of the present study was to determine the epidemiology of injuries associated with a wide array of nursery products among young children treated in US EDs. To our knowledge, this study is the first to comprehensively investigate nursery product–related injuries by using a nationally representative sample.
Methods
Data Source
The National Electronic Injury Surveillance System (NEISS),23 which is operated by the US Consumer Product Safety Commission (CPSC), monitors consumer product–related and sports and recreational activity–related injuries treated in US EDs.24 Approximately 100 hospitals, including 8 children’s hospitals, contribute to the NEISS, which represents a stratified probability sample of >5300 hospitals with a 24-hour ED with at least 6 beds in the United States and its territories.25,26 Professional NEISS coders abstract information from ED medical records, including patient demographic characteristics, the consumer product involved, injury diagnosis, affected body region, disposition from the ED, and a brief narrative regarding the circumstances of the incident.27
Nursery product–related injuries among children aged <3 years reported through the NEISS from 1991 through 2011 were retrospectively analyzed. Nursery product–related injuries were identified by using 39 discrete NEISS consumer product codes (Supplemental Information),24 which were based on the product codes included in the CPSC annual report on nursery product–related injuries and deaths.10 Each case narrative was then examined, and cases were excluded if the injury did not involve a nursery product or involved a motor vehicle crash, diaper rash, animal bite, dermatitis, or conjunctivitis. The final data set contained 48 653 actual cases.
Study Variables
NEISS case narratives were individually reviewed to identify the mechanism of injury, which was classified as follows: (1) fell spontaneously or due to actions of the patient; (2) fell due to actions of another person; (3) collision with or while using the product; (4) breathing related; (5) entrapment; (6) product failure, which includes product collapse or malfunction; (7) ingestion; (8) nonfatal submersion; and (9) other. In instances in which mechanisms of injury overlapped, the initial event in a sequence of events was considered the mechanism of injury. NEISS consumer product codes were regrouped into 12 major categories of nursery products, similar to categories used by the CPSC (Supplemental Information).10
The NEISS variable for age was regrouped into 0 to 5 months, 6 to 11 months, 12 to 17 months, 18 to 23 months, and 24 to 35 months. Injury diagnosis was categorized as follows: (1) ingestion; (2) aspiration; (3) burn; (4) laceration (including the NEISS categories of amputation, laceration, puncture, and nondental avulsion); (5) concussion/closed head injury (CHI), including internal organ injury to the head; (6) soft tissue injury, including crushing, contusion/abrasion, hematoma, and strain/sprain; (7) anoxia/submersion; (8) fracture; (9) dental injury; or (10) other, including dislocation, foreign body, nerve damage, hemorrhage, electric shock, poisoning, internal organ injury to non-head body regions, and other. Body region was grouped into: (1) upper extremity, including shoulder, elbow, upper arm, lower arm, wrist, hand, and finger; (2) lower extremity, including knee, upper leg, lower leg, ankle, foot, and toe; (3) trunk, including upper trunk, lower trunk, and pubic region; (4) head/neck; (5) face, including face, eye, mouth, and ear; and (6) other, including injury to >25% of the body. Disposition from the ED was categorized as: (1) treated and released; (2) hospitalized, including NEISS categories of treated and transferred, treated and admitted, and held for <24 hours for observation; (3) left against medical advice; and (4) fatality. Location of injury was grouped into home (including home, apartment/condo, and manufactured/mobile home) and other. Additional variables analyzed included sex and year.
Statistical Analysis
Data were analyzed by using SPSS version 20.0 (IBM SPSS Statistics, IBM Corporation) and SAS 9.3 (SAS Institute, Inc, Cary, NC) statistical software. National injury estimates were calculated by using sample weights provided by the CPSC.25,26,28 All data reported in the present article are stable national estimates unless otherwise noted. An estimate is considered unstable if the estimate is <1200 cases, the sample size is <20 cases, or the coefficient of variation is >30%. US Census Bureau July 1 intercensal and postcensal population estimates from 1991 to 2011 were used to calculate injury rates.29–31 Piecewise linear regression models were used to analyze the trends. Trends involving all nursery products (Fig 1) or baby walkers/jumpers/exercisers (Fig 2) were analyzed by using 2003 as a breakpoint, whereas concussion/CHI (Fig 3) trends were analyzed by using 2005 as a breakpoint. The estimated annual rate of change from the regression model, denoted by “m,” was reported along with the P value associated with the t test used to test for its statistical significance. Other analyses included the Rao-Scott χ2 test for association, and calculation of relative risk (RR) with a 95% confidence interval (CI). The level of significance for all statistical tests was α = 0.05. This study was approved by the institutional review board of The Research Institute at Nationwide Children’s Hospital.
Estimated annual number and rate of nursery product–related injuries among children aged <3 years treated in US EDs, NEISS 1991 to 2011.
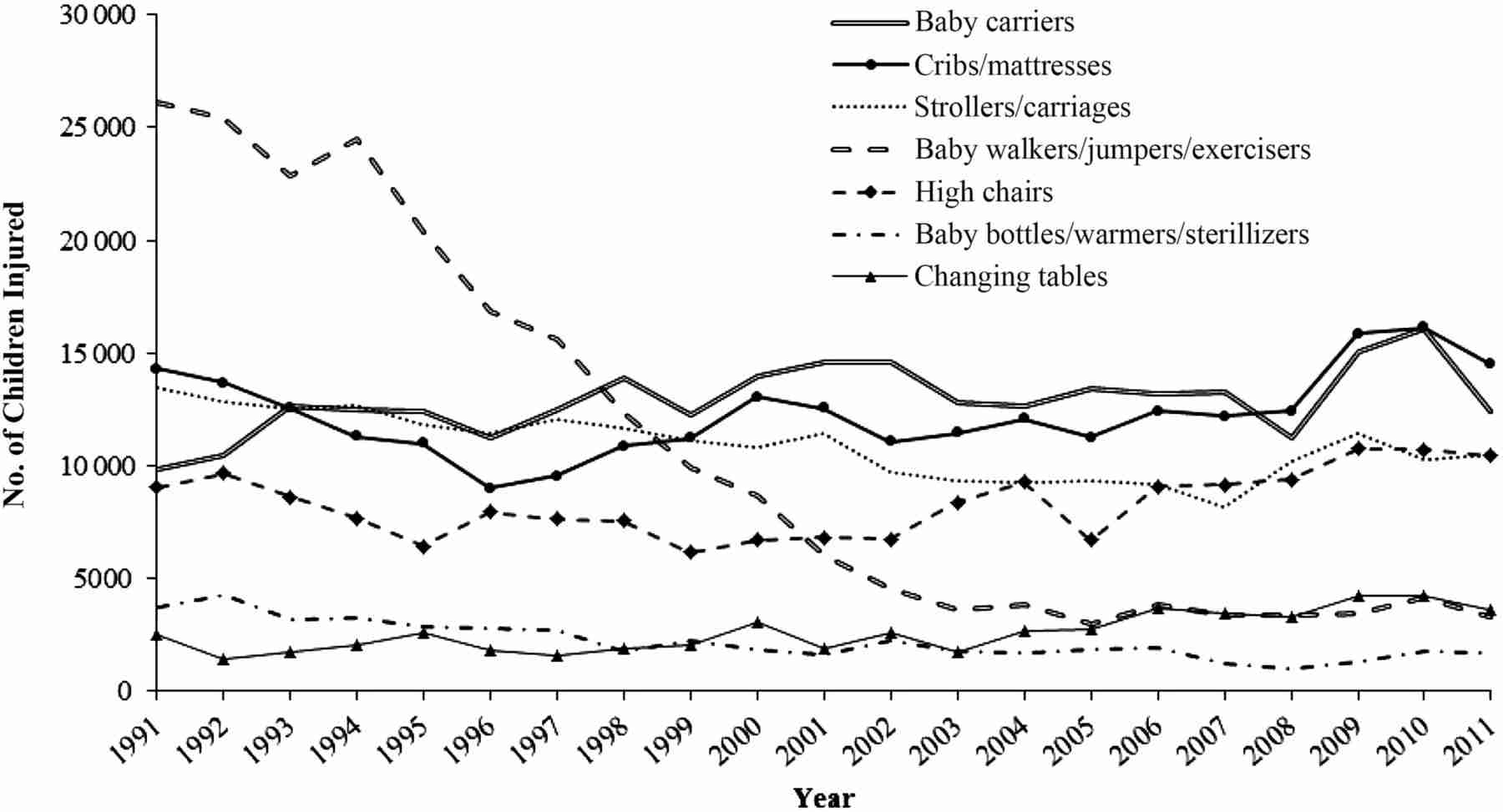
Estimated annual number of nursery product–related injuries among children aged <3 years according to selected nursery product categories, NEISS 1991 to 2011.
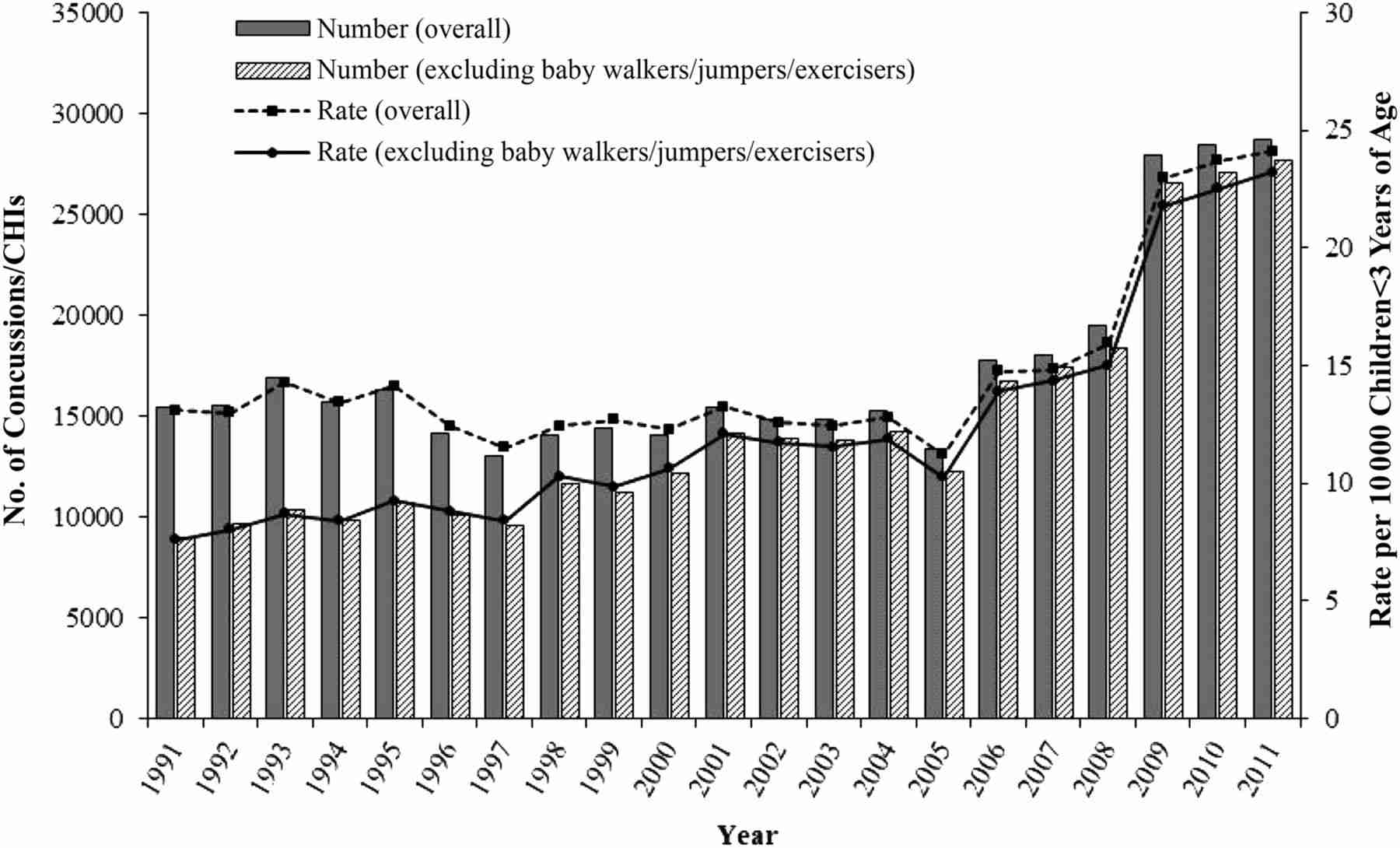
Estimated annual number and rate of concussions/CHIs associated with nursery products among children aged <3 years, NEISS 1991 to 2011.
Results
Demographic Characteristics
During the 21-year study period, an estimated 1 391 844 (95% CI, 1 169 489–1 614 199) children age <3 years were treated in US EDs for nursery product–related injuries, averaging 66 278 (95% CI, 55 690–76 867) injuries annually or 56.29 (95% CI, 47.30–65.29) injuries per 10 000 children. More than one-half (58.7%) of all injuries occurred during the first year of life, with infants 6 to 11 months old (35.5%) accounting for the highest proportion of injuries (Table 1). The median age of patients was 9.3 months (interquartile range, 5.3–15.3 months). More boys (54.9%) were injured than girls, and a majority of injuries occurred at home (87.9%).
Characteristics of Nursery Product–Related Injuries Treated in US EDs According to Age Group, NEISS 1991 to 2011
Injury Trends
There was a significant decline in both the annual number of nursery product–related injuries (–33.0%; m = –2323; P < .001) and the injury rate per 10 000 children <3 years old (–33.9%; m = –2.00; P < .001) from 1991 through 2003, after which both the number and rate increased significantly through 2011 by 23.5% (m = 2147; P < .001) and 23.7% (m = 1.52; P < .001), respectively (Fig 1). The main contributing factor to the decline was the decrease in the number of baby walker/jumper/exerciser-related injuries, which decreased significantly by 86.0% (m = –2051; P < .001) from 1991 to 2003, before leveling off (–8.9%; m = 114; P = .299) from 2003 through 2011 (Figs 1 and 2). Although several nursery product categories contributed to the overall increase observed after 2003 (Fig 2), there was no specific product category responsible for the trend. An increase in a diagnosis category (concussion/CHI), rather than a product category, was the main contributor to the observed increase in injuries during the latter part of the study period. The annual number (–12.9%; m = –113; P = .157) and rate (–14.2%; m = –0.12; P = .070) of nursery product–related concussions/CHIs did not decrease significantly from 1991 to 2005, and both the number (114.0%; m = 2667; P < .001) and rate (114.8%; m = 2.17; P < .001) increased significantly by >100% from 2005 through 2011 (Fig 3).
Injury Mechanism and Nursery Product Involved
A self-precipitated fall was the most common mechanism of injury (80.0%) (Table 2). Patients <6 months old were more likely to suffer injuries from a breathing-related mechanism (RR, 4.41 [95% CI, 3.48–5.60]), caregiver-related falls (RR, 5.98 [95% CI, 5.16–6.92), and product failure (RR, 3.02 [95% CI, 2.33–3.91]) than older patients. One- and two-year-old patients were more likely (RR, 2.52 [95% CI, 2.16–2.94]) to be injured from being entrapped in a product than patients <1 year old.
Characteristics of Nursery Product–Related Injuries According to Mechanism of Injury, Product Category, and Age Group, NEISS 1991 to 2011
Nursery product–related injuries were most commonly associated with baby carriers (19.5%), cribs/mattresses (18.6%), strollers/carriages (16.5%), and baby walkers/jumpers/exercisers (16.2%) (Table 2). These groups of nursery products also accounted for 86.1% of the injuries caused by self-precipitated falls. Baby carriers accounted for 54.0% of injuries among children <6 months old, and baby walkers/jumpers/exercisers accounted for 36.4% of injuries among children aged 6 to 11 months. Baby carriers were 5.52 times (95% CI, 4.61–6.60; 7.9% vs 1.4%) more likely to be related to a caregiver fall compared with other product groups, and they accounted for more than one-half (57.3%) of caregiver-related falls. Strollers/carriages (RR, 1.68 [95% CI, 1.35–2.08]; 3.6% vs 2.1%) and cribs/mattresses (RR, 3.18 [95% CI, 2.68–3.77]; 5.3% vs 1.7%) were associated with a greater risk of entrapment compared with other product categories. Product failure accounted for 0.9% of injuries, and almost one-half were associated with baby carriers (29.9%) or strollers/carriages (19.3%).
Body Region and Diagnosis
The head/neck was the most common body region injured (47.1%), followed by the face (34.0%) (Table 1). The proportion of head/neck injuries decreased with increasing age, whereas the proportion of upper and lower extremity injuries increased with increasing age. Patients <1 year old were more likely (RR, 1.63 [95% CI, 1.57–1.70]) to sustain an injury to the head/neck, and patients aged ≥1 year were more likely (RR, 3.33 [95% CI, 3.00–3.71]) to sustain an injury to the upper extremity compared with the other age group. The body region injured was not only associated with patient age but also with nursery product category and injury mechanism. Baby carriers, changing tables, portable baby swings, and baby bouncer seats combined were more likely (RR, 1.47 [95% CI, 1.41–1.54]; 61.6% vs 41.8%) to be associated with injuries to the head/neck compared with the other product groups. Strollers/carriages (RR, 1.34 [95% CI, 1.27–1.41]; 43.0% vs 32.1%) and baby bottles/warmers/sterilizers (RR, 1.92 [95% CI, 1.78–2.07]; 63.2% vs 32.9%) were more likely to be associated with facial injuries compared with other product groups. Entrapment was 6.70 (95% CI, 6.15–7.31; 56.6% vs 8.5%) times more likely to cause an upper extremity injury than other injury mechanisms.
Soft tissue injury (38.0%) and concussion/CHI (26.3%) were the most common diagnoses (Table 1). The proportion of injuries accounted for by concussion/CHI increased during the study period from 18.6% in 1991 to 41.9% in 2011. The proportion of concussions/CHIs decreased with increasing age, and the proportion of lacerations increased with increasing age. Patients ≥18 months old (RR, 2.17 [95% CI, 1.92–2.46]) were more likely to be diagnosed with a fracture, whereas patients <18 months old (RR, 1.74 [95% CI, 1.62–1.87]) were more likely to be diagnosed with a concussion/CHI compared with the other age group. The face was 7.00 (95% CI, 6.25–7.85; 38.2% vs 5.4%) times more likely to sustain a laceration; the upper and lower extremities (RR, 13.75 [95% CI, 11.91–15.87]; 34.0% vs 2.5%) combined were more likely to sustain a fracture compared with other body regions.
Disposition From EDs and Fatalities
Most (95.1%) children presenting to an ED with a nursery product–related injury were treated and released (Table 1). Of the patients admitted to the hospital (4.0%), 73.7% were <1 year old. Patients <6 months old were 2.11 times (95% CI, 1.81–2.46) more likely to be hospitalized than patients ≥6 months old. Baby carriers (25.8%), cribs/mattresses (19.5%), and baby walkers/jumpers/exercisers (18.7%) were most commonly associated with injuries requiring hospital admission. The breathing-related and nonfatal submersion mechanisms of injury combined were 6.56 (95% CI, 5.03–8.55; 24.9% vs 3.8%) times more likely to lead to hospitalization than the other mechanisms.
Of the 0.2% of injuries that resulted in death, 80.2% were among patients <1 year old, 86.9% were associated with the breathing-related mechanism, and 73.4% were associated with cribs/mattresses. Baby carriers were associated with an additional 10.1% of deaths.
Discussion
On average, >66 000 nursery product–related injuries were treated in the US EDs annually from 1991 through 2011. Despite the significant decline in both the number and rate of nursery product–related injuries from 1991through 2003, primarily attributable to the decline in baby walker/jumper/exerciser-related injuries, both the number and rate of injuries increased significantly from 2003 through 2011. Part of this increase was driven by an increase in the number and rate of concussions/CHIs, which is likely attributable to multiple factors, including heightened awareness about concussions during recent years among parents, child caregivers, and health professionals. These findings agree with a recent study, which reported a >200% increase in traumatic brain injuries among children aged <5 years occurring in the home from 1991 to 2012.32 Further research is needed to better define the factors contributing to the observed increase in concussions/CHIs.
From 2009 to 2012, nursery products were the leading children’s product category recalled in the United States,1–4 and it is estimated that up to 80% of recalled children’s products remain in consumer households after a recall.6 Since enactment of the Consumer Product Safety Improvement Act of 2008, which (among other requirements) mandated safety standards for all durable infant or toddler products,33 product recalls have begun to decline.6 However, components of the law are continuing to be phased-in, and its effects on nursery product–related injuries is unlikely to be reflected in the results of the present study. Future research is warranted to assess the effects of this important consumer product legislation on nursery product–related injuries to children.
Given the success of interventions to prevent injuries associated with baby walkers, including strengthened safety standards and new safer product design,18,20 similar efforts should be used to address injuries associated with other nursery products, especially the top contributors to pediatric morbidity in this study: baby carriers, cribs/mattresses, and strollers/carriages. Baby carriers were the leading source of nursery product–related injuries and hospital admissions. Baby carrier–related falls involving caregivers may lead to more severe injuries due to factors such as the caregiver falling on top of the child or propelling the child with additional momentum during a fall.34 To reduce the likelihood of these injuries, caregivers should attempt to keep living spaces free of objects that pose a tripping hazard. Child caregivers using a carrier should minimize the use of stairs and refrain from carrying other objects while on the stairs, using the free hand to grasp the handrail.35 Infants should be matched to carriers that are appropriate for their size and weight.36
Nearly one-third of product failures were associated with baby carriers, which included instances of handle detachment and product collapse. Baby carrier seats, especially detachable car seats, should be carefully inspected before infant transport. Any supporting devices and carrier handles should be locked into position before moving an infant or child.37 Carrier seats also pose an additional hazard of injuries due to unattended falls, which are associated with placement of seats on elevated surfaces.34,38 Infants in carrier seats should always be secured using the safety harness straps provided, and carriers should be equipped with nonskid undersides. Caregivers should not place carrier seats on slippery surfaces, such as glass tables, or on soft surfaces, such as beds, where a tip over could lead to suffocation.37
Cribs/mattresses were the second most common source of injury and were associated with the majority of nursery product–related fatalities. Previous literature provides evidence that cribs are a leading nursery product associated with infant mortality.15,22,39 It is likely that sudden unexpected infant death accounted for many of these fatalities in our study as well as in others. Sleep environment hazards play a key role in infant injury, especially sudden unexpected infant death, and health care practitioners should counsel caregivers to not place bumper pads or soft objects, such as blankets or pillows, in the crib because of the risk of strangulation, entrapment, and suffocation.36,37 Caregivers should only use the firm, snugly fitting mattress designed for their crib and never use supplemental mattresses, which may increase the risk of entrapment and suffocation.
Crib bumper pads have been marketed as protective barriers to reduce entrapment injuries, and some organizations, such as the Juvenile Products Manufacturers Association, maintain that bumper pads are safe.40 However, multiple fatalities attributable to bumper pad–related suffocation or strangulation have been reported.41,42 Since 2011, the American Academy of Pediatrics has recommended against bumper pad use due to the risk of injury.43,44 The city of Chicago45 and the state of Maryland46 have taken these recommendations further, banning the sale of bumper pads. Despite these public policy efforts, bumper pads can still be found in Chicago,47 and more needs to be done at the national level to limit the sale and use of crib bumper pads.
Strollers/carriages were the third-leading source of nursery product–related injuries. Tip overs and falls involving strollers have been described as the predominant mechanism of injury in the literature,12,48,49 underscoring the need for caregivers to avoid taking strollers on stairs, hanging objects on stroller handles, and allowing other children to play with or hang onto a stroller while a child is inside.36 These measures should be combined with safety belt use, which previous studies suggest is low among injured children.49 In a report describing stroller-related injuries in Queensland, Australia, researchers noted that 8% of fall injuries were due to the stroller rolling away from the caregiver.48 The injury risk from stroller-roll-away could be mitigated through the installation of a “dead man brake,” similar to those on airport trolleys. Manufacturers should be encouraged to place these conditional braking systems on child strollers and carriages.
Almost 90% of injuries occurred at home, and 80% of injuries were due to a fall. Therefore, prevention efforts should focus on fall prevention in the home setting. Strategies for preventing falls include the following: (1) use of products’ safety devices, such as a strap or harness; (2) appropriate adult supervision; and (3) proper assembly/installation and use of products, such as adjusting the mattress height in a crib to prevent a child from climbing out. We also found that young children were more likely to injure their head and neck or be diagnosed with a concussion/CHI, whereas older children were more likely to injure an upper extremity or be diagnosed with a laceration. This finding is most like due to children’s developmental changes and how this development specifically affects how they fall. Young children have disproportionately large heads, which provides a larger target for injury and also raises their center of gravity. These children tend to lead with their head when they fall and are unable to break their fall with their arms because of lack of coordination and strength. As they get older, they use their arms more effectively to protect their heads but have more upper extremity injuries as a result.32
Several limitations exist in this study. The number of nursery product–related injuries was underestimated because only cases treated in EDs were included. Injuries treated in urgent care centers and other non-ED medical facilities are not captured by the NEISS. Fatalities are also underreported in the NEISS because prehospital deaths may not be transported to an ED, and fatal patient outcomes after hospital admission are not captured in the NEISS database. The findings of this study, therefore, may not be representative of all nursery product–related injuries. In addition, NEISS case narratives are limited by the amount of detail included in ED medical records. Narratives may not consistently provide information about injury mechanism, factors contributing to the injury event, and which product was primarily involved in the injury if multiple products were listed. Information regarding socioeconomic status was unavailable. It is possible that some of these injuries were the result of child maltreatment. Because multivariate analyses were not performed, our results do not reflect the potential influence of covariates on the relationships examined. Despite these limitations, the strength of this study lies in its use of a large, nationally representative sample over a period of 21 years that includes product-specific information.
Conclusions
To our knowledge, this study is the first to use a nationally representative database to examine pediatric injuries associated with a wide array of nursery products. Although nursery product–related injuries declined from 1991 to 2003, primarily due to successful injury prevention efforts with baby walkers, these injuries increased during the final 8 years of the study (2003–2011). Greater efforts are warranted to prevent injuries associated with other nursery products, especially baby carriers, cribs, and strollers. Prevention of falls and concussions/CHIs associated with nursery products also deserves special attention. Future studies that further examine the circumstances of nursery product–related injuries and evaluate current safety interventions are needed to help inform the development of effective prevention strategies.
Footnotes
- Accepted January 6, 2017.
- Address correspondence to Gary A. Smith, MD, DrPH, Center for Injury Research and Policy, The Research Institute at Nationwide Children’s Hospital, 700 Children’s Dr, Columbus, OH 43205. E-mail: gary.smith{at}nationwidechildrens.org
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
References
- Copyright © 2016 by the American Academy of Pediatrics
In this issue

{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.