A randomized trial of the effect of patient race on physicians' intensive care unit and life-sustaining treatment decisions for an acutely unstable elder with end-stage cancer
- PMID: 21460710
- PMCID: PMC3119368
- DOI: 10.1097/CCM.0b013e3182186e98
A randomized trial of the effect of patient race on physicians' intensive care unit and life-sustaining treatment decisions for an acutely unstable elder with end-stage cancer
Abstract
Objectives: To test whether hospital-based physicians made different intensive care unit and life-sustaining treatment decisions for otherwise identical black and white patients with end-stage cancer and life-threatening hypoxia.
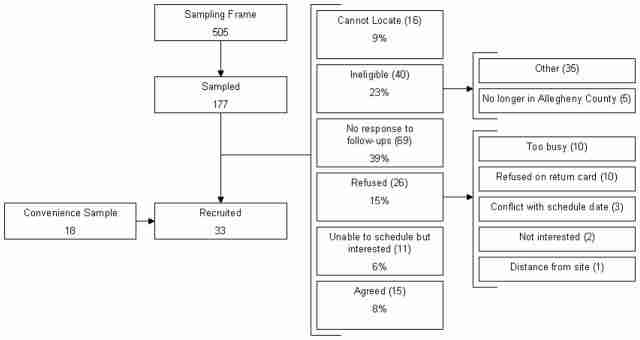
Design: We conducted a randomized trial of the relationship between patient race and physician treatment decisions using high-fidelity simulation. We counterbalanced the effects of race and case by randomly alternating their order using a table of random permutations. Physicians completed two simulation encounters with black and white patient simulator patients with prognostically identical end-stage gastric or pancreatic cancer and life-threatening hypoxia and hypotension, followed by a self-administered survey of beliefs regarding treatment preferences by race. We conducted within-subjects analysis of each physician's matched-pair simulation encounters, adjusting for order and case effects, and between-subjects analysis of physicians' first encounter, adjusting for case.
Setting: Peter M. Winter Institute for Simulation Education and Research at the University of Pittsburgh, Pennsylvania.
Subjects: Thirty-three hospital-based attending physicians, including 12 emergency physicians, eight hospitalists, and 13 intensivists from Allegheny County, Pennsylvania.
Intervention: Race of patient simulator.
Measurements and main results: Measurements included physician treatment decisions recorded during the simulation and documented in the chart and beliefs about treatment preference by race. When faced with a black vs. a white patient, physicians did not differ in their elicitation of intubation preferences (within-subject comparison, 28/32 [88%] vs. 28/32 [88%]; p = .589; between-subject comparison, 13/17 [87%] vs. 13/17 [76%]; p = .460), intensive care unit admission (within-subject comparison, 14/32 [44%] vs. 12/32 [38%]; p = .481; between-subject comparison, 8/15 (53%) vs. 7/17 (41%); p = .456), intubation (within-subject comparison, 5/32 [16%] vs. 4/32 [13%]; p = .567; between-subject comparison: 1/15 [7%] vs. 4/17 [24%]; p = .215), or initiation of comfort measures only (within-subject comparison: 16/32 [50%] vs. 19/32 [59%]; p = .681; between-subject comparison: 6/15 [40%] vs. 8/17 [47%]; p = .679). Physicians believed that a black patient with end-stage cancer was more likely than a similar white patient to prefer potentially life-prolonging chemotherapy over treatment focused on palliation (67% vs. 64%; z = -1.79; p = .07) and to want mechanical ventilation for 1 wk of life extension (43% vs. 34%; z = -2.93; p = .003), and less likely to want a do-not-resuscitate order if hospitalized (51% vs. 60%; z = 3.03; p = .003).
Conclusions: In this exploratory study, hospital-based physicians did not make different treatment decisions for otherwise identical terminally ill black and white elders despite believing that black patients are more likely to prefer intensive life-sustaining treatment, and they grossly overestimated the preference for intensive treatment for both races.
Figures
{kind=link}
Comment in
-
Innovative research on end-of-life decision making.Crit Care Med. 2011 Jul;39(7):1831-2. doi: 10.1097/CCM.0b013e31821caf33. Crit Care Med. 2011. PMID: 21685750 No abstract available.
Similar articles
-
Using simulation to isolate physician variation in intensive care unit admission decision making for critically ill elders with end-stage cancer: a pilot feasibility study.Crit Care Med. 2008 Dec;36(12):3156-63. doi: 10.1097/CCM.0b013e31818f40d2. Crit Care Med. 2008. PMID: 18936694 Free PMC article.
-
Differences in Physicians' Verbal and Nonverbal Communication With Black and White Patients at the End of Life.J Pain Symptom Manage. 2016 Jan;51(1):1-8. doi: 10.1016/j.jpainsymman.2015.07.008. Epub 2015 Aug 20. J Pain Symptom Manage. 2016. PMID: 26297851 Free PMC article. Clinical Trial.
-
Physicians' decision-making roles for an acutely unstable critically and terminally ill patient.Crit Care Med. 2013 Jun;41(6):1511-7. doi: 10.1097/CCM.0b013e318287f0dd. Crit Care Med. 2013. PMID: 23552510 Free PMC article. Clinical Trial.
-
The effects of patient race on outcomes in seriously ill patients in SUPPORT: an overview of economic impact, medical intervention, and end-of-life decisions. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments.J Am Geriatr Soc. 2000 May;48(S1):S194-8. doi: 10.1111/j.1532-5415.2000.tb03132.x. J Am Geriatr Soc. 2000. PMID: 10809475 Review.
-
Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities.J Gen Intern Med. 2013 Nov;28(11):1504-10. doi: 10.1007/s11606-013-2441-1. Epub 2013 Apr 11. J Gen Intern Med. 2013. PMID: 23576243 Free PMC article. Review.
Cited by 17 articles
-
Psychological Attachment Orientations of Surrogate Decision-Makers and Goals-of-Care Decisions for Brain Injury Patients in ICUs.Crit Care Explor. 2020 Jul 6;2(7):e0151. doi: 10.1097/CCE.0000000000000151. eCollection 2020 Jul. Crit Care Explor. 2020. PMID: 32696015 Free PMC article.
-
Association between Chinese or South Asian ethnicity and end-of-life care in Ontario, Canada.CMAJ. 2020 Mar 16;192(11):E266-E274. doi: 10.1503/cmaj.190655. CMAJ. 2020. PMID: 32179535 Free PMC article.
-
Estimating ICU Benefit: A Randomized Study of Physicians.Crit Care Med. 2019 Jan;47(1):62-68. doi: 10.1097/CCM.0000000000003473. Crit Care Med. 2019. PMID: 30303839 Free PMC article.
-
End-of-Life Plans for African American Older Adults With Dementia.Am J Hosp Palliat Care. 2018 Oct;35(10):1314-1322. doi: 10.1177/1049909118761094. Epub 2018 Mar 14. Am J Hosp Palliat Care. 2018. PMID: 29540073 Free PMC article.
-
Hospital-Based Physicians' Intubation Decisions and Associated Mental Models when Managing a Critically and Terminally Ill Older Patient.Med Decis Making. 2018 Apr;38(3):344-354. doi: 10.1177/0272989X17738958. Epub 2017 Nov 22. Med Decis Making. 2018. PMID: 29166565 Free PMC article.
Publication types
MeSH terms
Grant support
LinkOut - more resources
-
Full Text Sources
-
Other Literature Sources
-
Medical